

Troubled Waters Reading Urine in Medieval Medicine
From cabbage green to course meal, medieval manuscripts exhibit a spectrum of colours and consistencies when describing urine. Katherine Harvey examines the complex practices of uroscopy: how physicians could divine sexual history, disease, and impending death by studying the body's liquid excretions.
April 19, 2023
 Scroll through the whole page to download all images before printing.
Scroll through the whole page to download all images before printing.Woodcut uroscopy chart pairing urine flasks with colour descriptions, printed at the private press of Ulrich Pinder, physician to the City of Nuremberg, 1506 — Source.
In the mid-thirteenth century, William of Rubruck, a Flemish Franciscan friar, travelled to the Mongol Empire. The main purpose of his visit was to undertake missionary work, but he also wrote a colourful account of his travels for King Louis IX of France, in which he described the region and its inhabitants. Among his many curious observations, he was astonished to find that the local physicians, who were generally skilled and knowledgeable, did not examine their patients’ urine.1
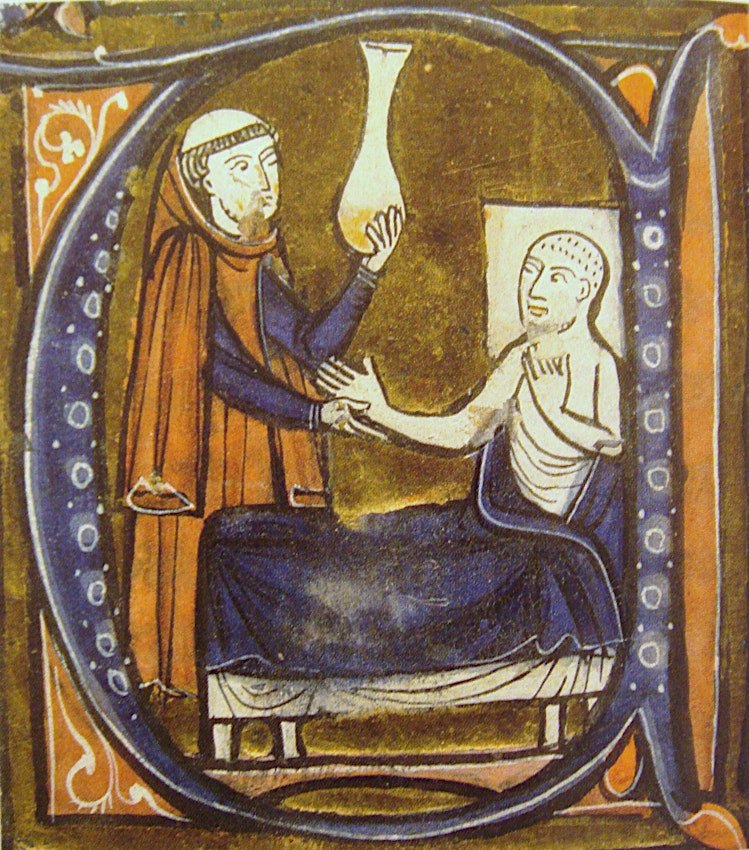
To the modern reader, this seems an odd detail to highlight, but William came from a world in which uroscopy — the examination of urine for the purpose of diagnosis and prognosis — was one of a doctor’s most valued skills. The link was so strong that the urine flask became the identifying symbol of the late medieval physician, who was often shown examining a sample. The symbol was used both to celebrate illustrious figures such as St Cosmas (the patron saint of medicine), and to punish charlatans like Roger Clerk of Wandsworth, who in 1382 was found guilty of selling useless “cures” to the poor, despite having no medical knowledge or training. He was led to the pillory on a saddleless horse, “a urinal being hung before him, and another urinal on his back”, in mockery of his malpractice. Satirists jeered at practitioners for their obsession with such unsavoury matter (Petrarch memorably claimed that the papal physicians were pale and emaciated because they “rummage around in sloshing chamber pots”), and comic images of monkey-physicians examining urine flasks are found in both manuscript marginalia and in early fourteenth-century stained glass at York Minster.2
Medieval physicians were interested in their patients’ urine because it provided immediate insight into the humoral state of the body. Before William Harvey discovered the circulation of the blood in the seventeenth century, physicians believed that the principal purpose of digestion was to convert food into blood, which was constantly being used up, and thus had to be replenished every night while the patient slept. Digestion was a complex, multi-stage process, and it led to various waste products like urine, which bore traces of the organs involved in its production (including the stomach, intestines, liver, and kidneys). Consequently, if the body was too hot or too cold, or if its humours were out of balance, this would be apparent from the urine it produced.3
 Scroll through the whole page to download all images before printing.
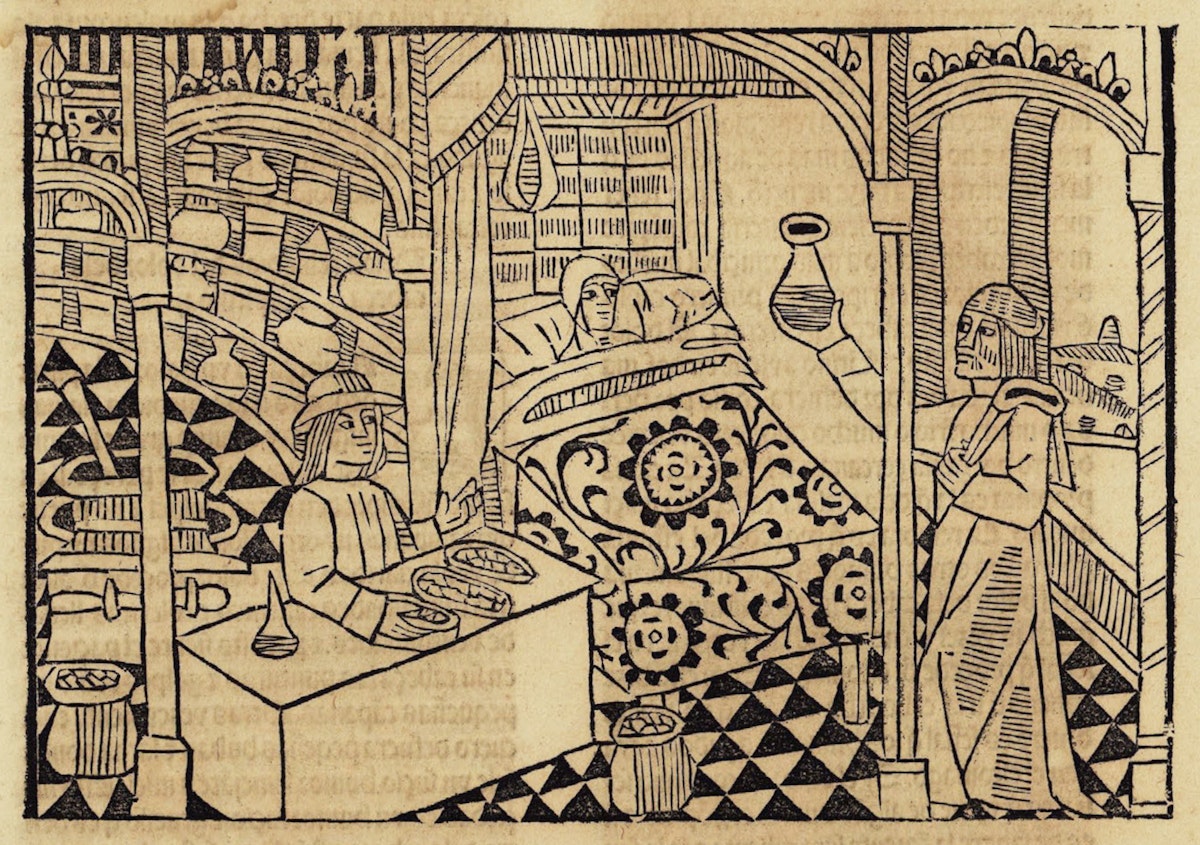
Scroll through the whole page to download all images before printing.Woodcut of a physician examining the “causes and signs” of disease, holding a urine flask up to the light, from a Spanish manuscript of Bartholomaeus Anglicus’ De proprietatibus rerum, ca. 1494 — Source.
 Scroll through the whole page to download all images before printing.
Scroll through the whole page to download all images before printing.Uroscopy is a very old practice, dating back at least as far as the ancient Babylonians, and was widely discussed by the classical authorities whose writings formed the basis of much medieval medical practice. The Hippocratic Aphorisms include advice on urine-based diagnosis and prognosis. For example: “Colourless urine is bad; it is especially common in those with disease on the brain” and “The presence of particles like coarse meal in the urine of patients with fever signifies a long illness”.4 Over the centuries, a substantial literature on the subject accumulated, and the Articella — a collection of treatises that formed the basis of university medical education in the later middle ages — included Isaac Judaeus’ Liber Urinarum (written in the ninth century) and De urinis by Giles of Corbeil (ca. 1140–1220). Since uroscopy lent itself to diagrammatic representation, practising physicians often used illustrated guides: such texts survive in sufficient numbers to suggest that they were widely-employed working tools in later medieval Europe.
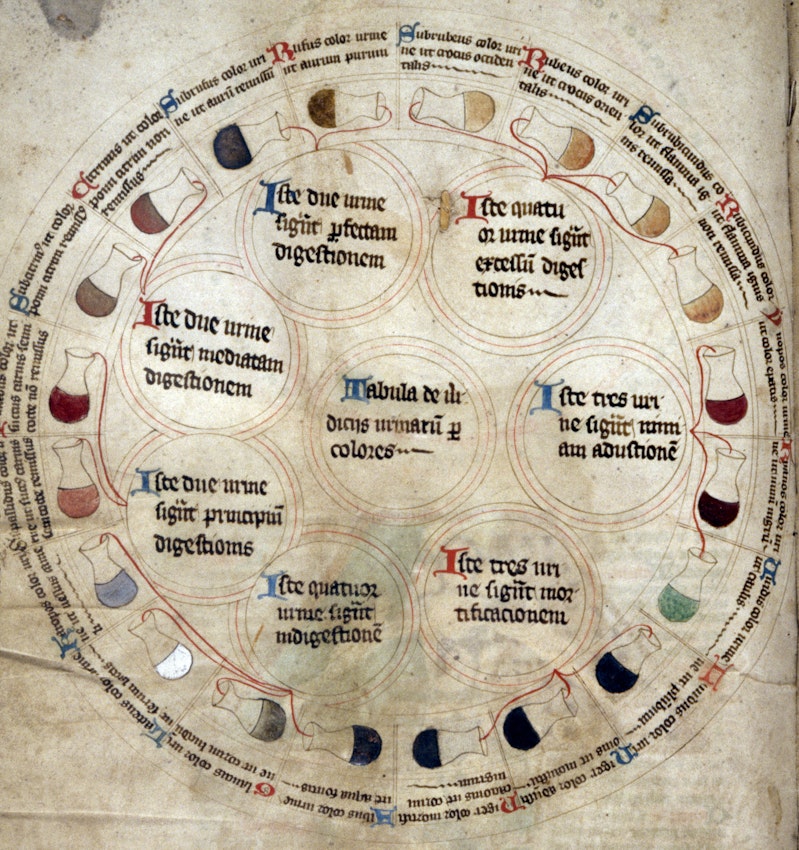
A particularly fine example is found in Bodleian Library MS Savile 39, which includes a late fourteenth-century ring diagram complete with twenty labelled flasks, their colours ranging from white to black. The flasks are grouped according to meaning: four reddish-gold samples, for example, signify good digestion, whilst three flasks of very dark liquid suggest death. Some authors are quite imaginative in their description of the colours: in a late fifteenth-century miscellany, one sample is described as being “green like cabbage”. Another widely circulated treatise described a “type of black urine that is caused by mortification, and that type of blackness is most like a polished black horn, or like a raven’s feather, or like a man from Ethiopia”.5 Such comparisons to familiar sights were probably intended to help practitioners distinguish between very similar colours, and to compensate for the shortcomings of the diagrams, the decoration of which sometimes owed more to the availability of pigments than to scientific accuracy.
 Scroll through the whole page to download all images before printing.
Scroll through the whole page to download all images before printing.Medical ring diagram with urine flasks from MS Savile 39, ca. 1387–1400 — Source.
 Scroll through the whole page to download all images before printing.
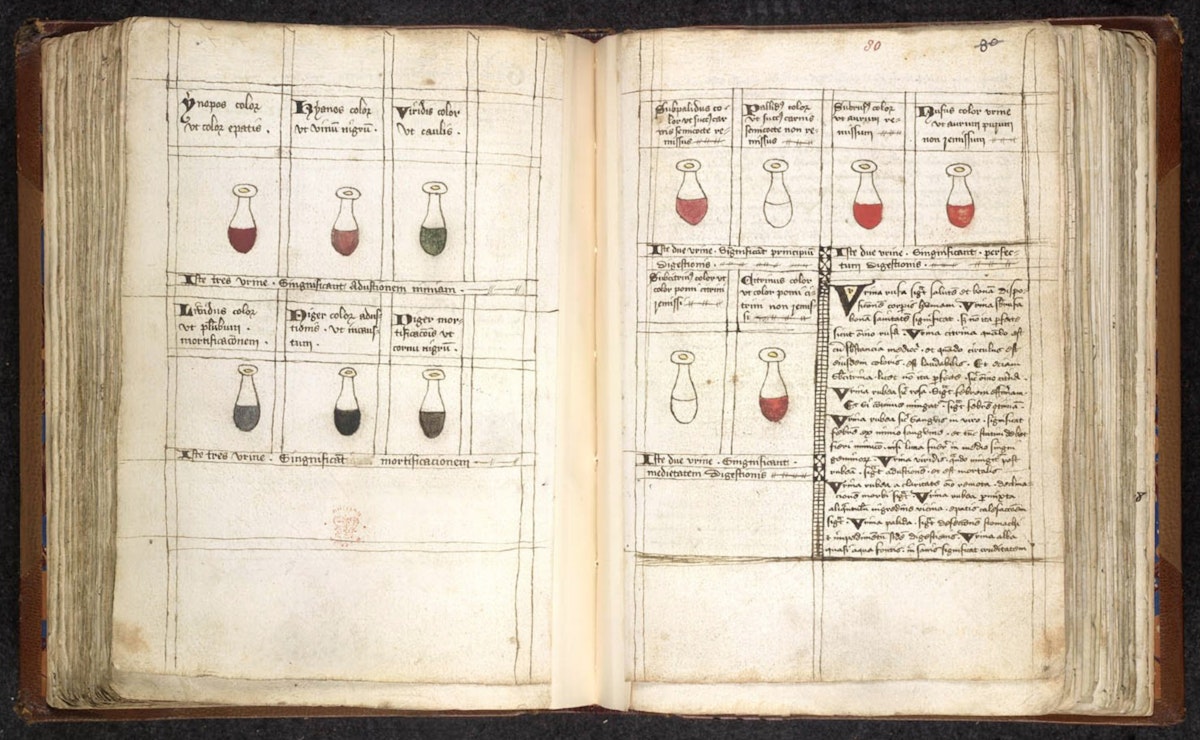
Scroll through the whole page to download all images before printing.Pages on interpreting the colour of urine from Sloane 1313, a Latin and French medical miscellany, ca. 1500–1600 — Source.
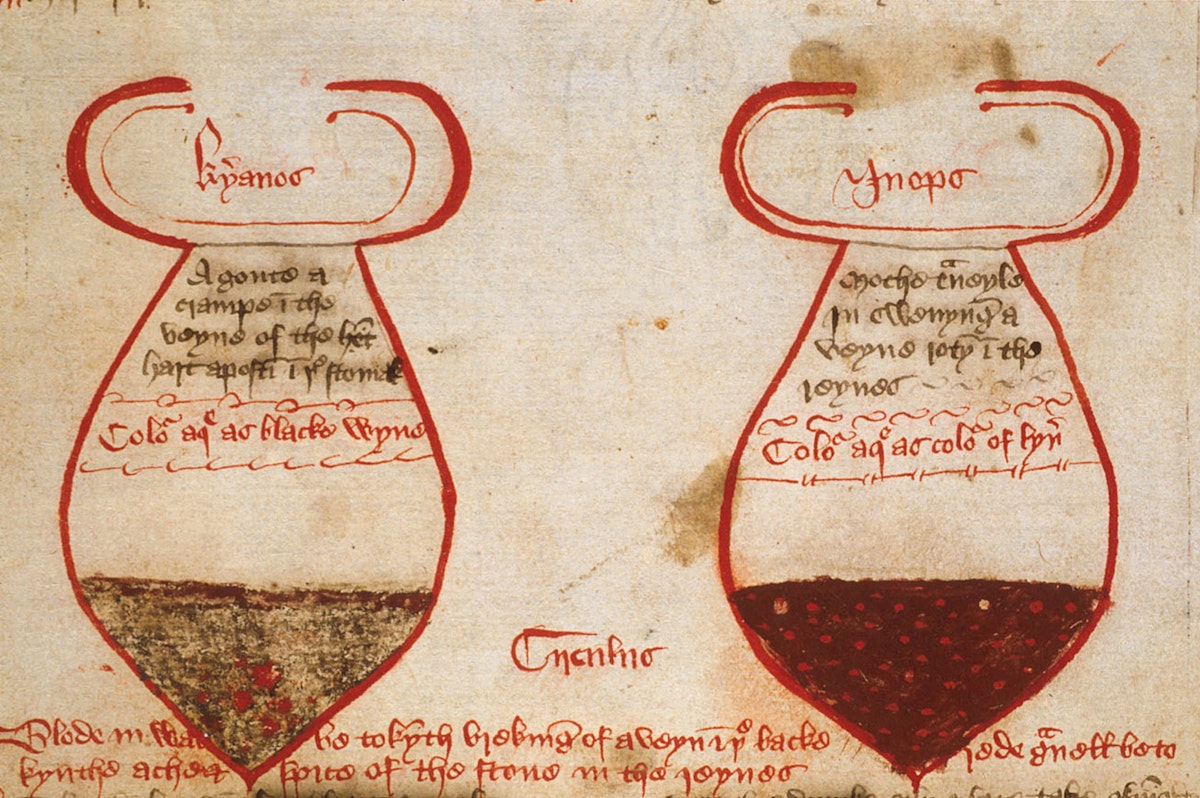
Many treatises suggested that it was possible to identify several layers in the urine, which meant that some diagrams show samples with very distinctive (and surely exaggerated) colour differences: red with a mint-green layer on top, or olive green with an orange-ish ring. If the top layer was particularly large, it might signify head pain; if it was very foamy, that indicated “gassiness boiling into the urinary vessels or distension or some other disorder of the lung”. The middle region should be examined for cloudiness, which could be a good or a bad sign depending on the condition from which the patient was suffering. It was at the bottom of the sample that one was most likely to see sediments, although these might also be suspended in the urine.6 Some texts place particular emphasis on things found in urine: in this pair of flasks, from an early fifteenth-century medical miscellany, we can see blood in one sample, and particles suspended in the other. The captions explain the meaning of these worrying features: blood in the urine indicates a broken vein at the back of the head, and gravel “betokeneth ache and spite of the stone in the reynes” — that is, kidney stones.
 Scroll through the whole page to download all images before printing.
Scroll through the whole page to download all images before printing.Manuscript detail from Sloane 7, a medical miscellany showing urine flasks with different layers of colour and particles, ca. 1400–25. The left is labelled “kyanos” (blue) in Greek and the right is labelled “inopos” (wine-coloured) — Source.
To interpret all these signs correctly, the skilled physician would not simply match the sample to the colour swatch; rather, he would combine his observations with his own extensive knowledge (both theoretical and practical) in order to identify what ailed his patient and determine the likely progression of his or her disease. Surprisingly often, this was done remotely: such was the trust in this method that many patients simply sent a sample to the doctor, who examined it and sent his verdict back. In 1334, the Aragonese towns of Vic and Montcada agreed to share a municipal physician, even though they are some sixty kilometres apart. The man appointed, Romon Ardey, was to live in Vic, but to interpret urines brought to him from either town.7 Far from being a strategy restricted to those who could not afford to see a doctor, this form of consultation was used even by the wealthiest members of society, such as Agnes, Lady Stonor, who in 1480 “sente here water unto M. Derworthe to undirstonde his conceite, ande howe he demyth by her water whedir she be in wey of mending”. His verdict is not recorded, but she died the following year.8
Not everyone thought this was a good idea: Isaac Judaeus, author of one of the most authoritative uroscopy treatises, criticised “fools who would base prophecies on it, without seeing the patient, and determine what disease is present, and whether the patient will die, and other foolishness”.9 Anyone who did consult in this way should obtain as much contextual information as possible, to avoid falling into the same trap as the eminent Parisian physician Guillaume Boucher (d. 1410). He examined a sample, and confidently announced that it belonged to a man with stomach problems. The couriers burst out laughing, because it was produced by a woman.10 Partly motivated by a desire to avoid such humiliation, university-educated physicians increasingly argued that bedside medicine was the best form of treatment: it allowed the practitioner to conduct a physical examination (considering other important signs, such as pulse, and scrutinising other excreta, such as sweat and faeces) and to interrogate the patient about his symptoms.11
Bedside medicine also allowed the physician to assert authority by showing off his knowledge and skills — something which most were very keen to do, in order to prove their superiority over their many rivals on the medical marketplace. Examining a urine sample in the presence of the patient who produced it, plus his family, friends, or servants, could be a particularly effective way to do this, as the process was straightforward but impressive. Ideally, the sample was collected in the morning, after the patient had slept and before he drank anything, and then allowed to settle for several hours; during this time, it must not be exposed to direct sunlight or excessive heat, which might change its composition.12 The physician’s inspection typically took place towards the end of his visit, and he often made a performance of it, holding the flask up to the light, and scrutinising it at length. One twelfth-century manual suggested that “While you look at the urine for a long time you pay attention to its colour, substance and quantity and to its contents from the diversity of which you will diagnose the different kinds of diseases . . . whereupon you promise health to the patient who is hanging on your lips.”13
 Scroll through the whole page to download all images before printing.
Scroll through the whole page to download all images before printing.Detail from a French miniature depicting scenes of medical consultation, including a physician examining a urine flask (top right), ca. 1300–1325 — Source.
 Scroll through the whole page to download all images before printing.
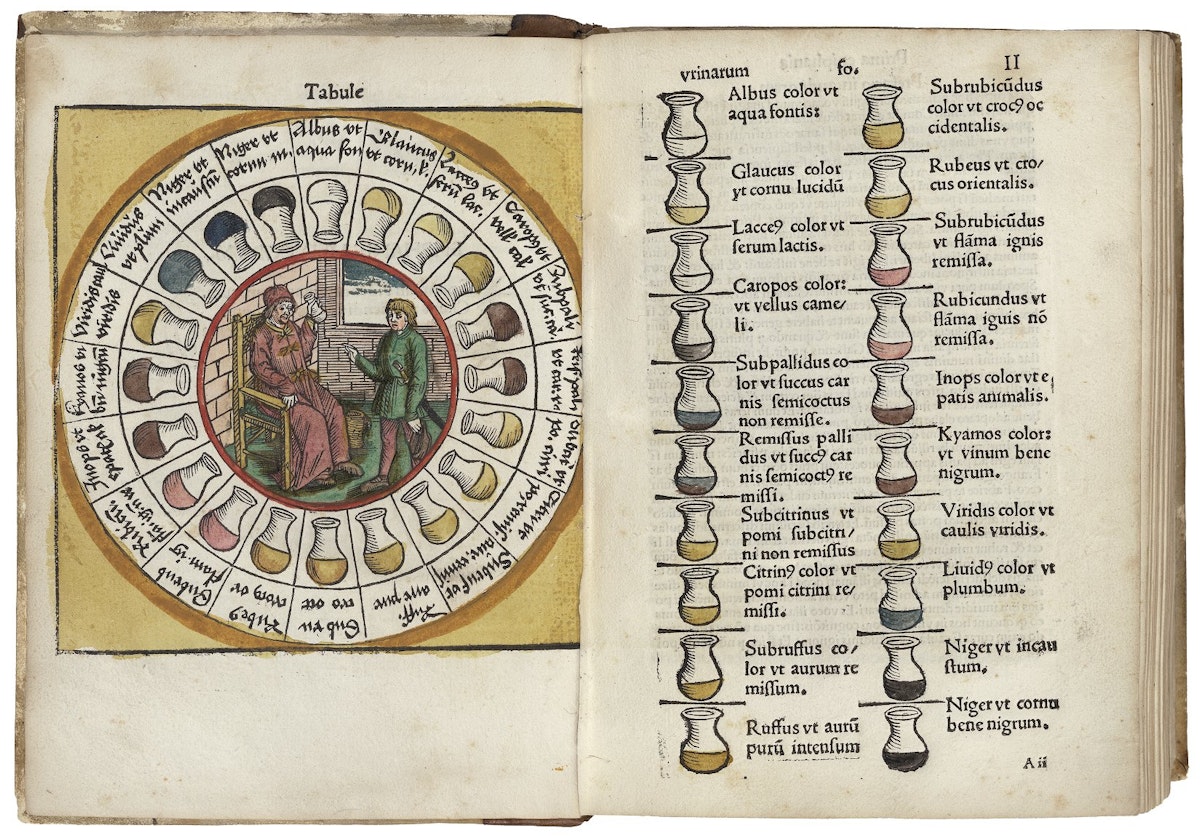
Scroll through the whole page to download all images before printing.Woodcut uroscopy diagnostic chart, printed at the private press of Ulrich Pinder, physician to the City of Nuremberg, ca. 1506 — Source.
A skilled physician could identify a whole range of conditions based on a urine sample. According to Giles of Corbeil’s influential treatise, pure and unclotted blood in the urine indicated a problem with the kidneys, especially if it was accompanied by pain; “lividity coupled with minute, distinct particles consistently indicates respiratory trouble”, and gout was revealed by “tiny white flecks”.14 Urine was a particularly useful tool for diagnosing leprosy, because the immediate physiological cause was thought to be a malfunctioning liver — an organ which was central to the digestive process, and thus any problems would be visible in the urine. In 1456, when Richard Walsham, a monk of Norwich Cathedral Priory, was suspected of contracting leprosy, the Prior had several physicians examine his body and urine in order to confirm that he was not afflicted.15
Medieval people also believed that uroscopy could reveal when an individual would die, allowing him to use his final days wisely. After William the Conqueror fell from his horse in 1087, he suffered agonising internal injuries. According to the chronicler William of Malmesbury (ca. 1090–1143), his physicians “inspected his urine and foretold certain death”, which allowed him to receive the last rites and to put his affairs in order.16 In 1214, suspecting that he was fatally ill, Abbot John of St Albans examined his own urine for “the small, hidden marks which he knew to be signs of death”, and correctly predicted that he had only three days to live. The Abbey’s chronicler admiringly noted that being “very experienced in the art of medicine, [John] had often made similar infallible predictions . . . about others.”17
 Scroll through the whole page to download all images before printing.
Scroll through the whole page to download all images before printing.Detail of a miniature depicting the bedridden John, Duke of Normandy, and physicians examining his urine, ca. 1380–1400 — Source.
Urine predicted the end of life, but it could also be used to track its conception through fertility testing. The Trotula, an influential compendium of women’s medicine, recommended that both husband and wife should urinate in a pot of bran: if, after ten days, either pot was stinking and full of worms, that indicated which spouse was infertile.18 According to The Dome of Uryne (a widely circulated Middle English compendium of uroscopic texts), it was possible to know whether a woman had conceived immediately after intercourse: if her urine was clear, then she was pregnant, and if it was thick, she was not. A few months on, the sex of the child could be determined by the cloudiness of the mother’s urine, whilst lead-coloured urine suggested a miscarriage.19 But not all physicians were willing to pronounce on such matters. A wise one would refuse to do so if he suspected that a female patient was intending to procure an abortion.20
Urine could be used to uncover an individual’s sexual history. The water of a “constant virgin” would be “wan and extremely calm”, and passed in a slow, delicate fashion because the passages of the womb and vulva were narrow. (It was evidently common to conflate the urinary passage and vagina.) On the other hand, “Thick urine of a woman declares her to be corrupt”. Men’s urine could be equally revealing, as seed in the bottom of the flask proved that the provider recently had sex.21 In the mid-twelfth century, shortly after taking his third wife, Ralph, Count of Vermandois, became seriously ill, and his doctor told him to abstain from marital relations. But when the physician examined the count’s urine, he realised that his advice had been ignored, and correctly predicted that Ralph would be dead within three days.22
Count Ralph’s unfortunate demise highlighted another potential problem with uroscopy: patients who ignored or mistrusted their doctors. Some went so far as to test the skills of their chosen practitioner. Although Arabic medical authorities such as Rhazes and Avicenna — both of whom were widely read and highly respected in the medieval West — recommended it, European physicians rarely smelt or tasted urine for medical reasons.23 Even so, they might be well-advised to give it a discreet sniff, since cynical patients sometimes provided samples of white wine or other yellowish liquids.24 In one extreme case from around the year 1000, the duke of Bavaria began his consultation with the famous monk-physician Notker by sending him a urine sample provided not by the duke, but by a pregnant servant girl. On examining it, Notker fell to his knees, praising God and declaring: “Within the week, the Lord will perform an unheard-of miracle: the duke will give birth to a son!” Shortly afterwards, the maid produced a baby boy, and the duke sent his messengers back to Notker with a sample of his own.25
 Scroll through the whole page to download all images before printing.
Scroll through the whole page to download all images before printing.Illumination of the Perisan physician Rhazes (Abu Bakr Mohammad Ibn Zakariya al-Razi) practising uroscopy, from a manuscript of Gerard of Cremona’s Recueil des traités de médecine, ca. 1250–1260 — Source.
In theory, patients could also fall victim to urine-related trickery, as happens in a humorous tale from The Decameron in which Calandrino’s friends team up with a doctor to convince him he is pregnant.26 But for the most part, the demand and trust in uroscopy was high, because it seemed to offer objective and certain diagnosis for a relatively small cost. In 1315, when Jaume II of Aragon closed a street in Barcelona’s Jewish quarter, he exempted the physician Vidal Rouen, because “many people have to show him the urines of sick people and to ask him for advice for them”.27 Other towns in the region appointed municipal physicians for this purpose: Abraham des Castlar, employed in this capacity by Castelló d’Empúries in 1316, agreed to “look at and assess all the urines brought to me by the citizens”.28
Indeed, the demand for uroscopy was too high to be satisfied by university-trained physicians (who were both rare and expensive), and many patients turned to less qualified practitioners. In mid-fifteenth century Essex, John Crophill worked as both a bailiff and a healer. Seemingly self-taught, and certainly not university educated, his commonplace book includes two texts on urine (alongside others on subjects such as blood-letting and astrology), plus a list of patients whose urine he had examined, and to whom he had provided cures.29 Across the Channel, Jacoba Felice, an unlicensed female practitioner who appeared before the Parisian medical authorities in 1322, offered similar services. Several of her mostly female clientele recalled her “continually examining their urine in the manner of physicians and doctors”, and reported that she had cured them when male physicians had failed to do so.30 Eighteen years earlier, when Gueraula de Codines faced a similar hearing in Barcelona, she asserted that “she could diagnosis a patient’s illness from his urine”, having been taught to do so by “a certain foreign doctor”. Clearly her legal travails did not deter patients, since three years later, she was back in court, claiming that many people consulted her, and that her uroscopy skills were especially in demand.31
Whilst professional trust in uroscopy waned considerably after ca. 1500, partly because of its growing association with such quacks, patient enthusiasm for this cheap, convenient, and reliable practice remained high.32 Indeed, although uroscopy no longer serves as an all-purpose diagnostic tool, new forms of urine analysis have developed from these ancient traditions, and our present-day medical landscape is awash with urine samples. Although twenty-first century patients benefit from relatively recent innovations such as hormone-based pregnancy tests, colour is still used to diagnose conditions including porphyria, whilst bloody and/or cloudy urine continues to be recognised as a sign of kidney stones and infections. Although medieval understandings of urine were deeply flawed, the popularity and longevity of urine-based diagnosis reflect an enduring desire on the part of both patients and physicians for reliable tests which provided objective diagnoses, and serve as an important reminder that, contrary to popular stereotypes of pre-modern medicine, much of it was rational, methodical, and rooted in science.
- Life of Pee: The Story of How Urine Got Everywhere
Alchemists sought gold in it. David Bowie refrigerated it to ward off evil. In the trenches of Ypres soldiers used it as a gas mask, whereas modern-day terrorists add it to home-made explosives. All the Fullers, Tuckers, and Walkers in the phonebook owe their names to it, and in 1969 four bags for storing it were left on the surface of the moon. In Life of Pee Sally Magnusson unveils the secret history of civilisation’s most unsavoury and unsung hero, and discovers how our urine footprint is just as indelible as our carbon one.
- Medicine Before the Plague: Practitioners and their Patients in the Crown of Aragon 1285–1345
This book describes the medical world of the early fourteenth century through a study of the extensive archival material and contemporary writings which exist for eastern Spain in the decades before the Black Death. It describes the range of medical practice which then existed — a continuum ranging from scattered academic physicians to barbers and empirics — and gives evidence for the levels and numerical growth of these various occupations in early fourteenth-century communities.
- The Dome of Uryne: A Reading Edition of Nine Middle English Uroscopies
This volume contains nine of the most widely disseminated Middle English uroscopies, each of them short enough to be consulted quickly by practitioners and all of them commonly found in English medical miscellanies. Practical in their orientation, they are grounded firmly in Galenic humoralism and derive directly and indirectly from canonical Latin uroscopies, along with the Arabic and Greek antecedents of the Latin tradition. Together they occur in over 120 manuscripts.

The Public Domain Review receives a small percentage commission from sales made via the links to Bookshop.org (10%) and Amazon (4.5%). Thanks for supporting the project! For more recommended books, see all our “Further Reading” books, and browse our dedicated Bookshop.org stores for US and UK readers.
Katherine Harvey is a UK-based historian, writer and reviewer, specialising in medieval history. She holds a BA, MA and PhD in History from King’s College London, is an Honorary Research Fellow at Birkbeck, University of London, and teaches for both Birkbeck and the Open University. She has published widely in both academic journals and popular periodicals, including BBC History Magazine, History Today, Aeon and The Atlantic. She reviews regularly for publications including the The Sunday Times and The Times Literary Supplement. Her most recent book, The Fires of Lust: Sex in the Middle Ages, was published by Reaktion in October 2021.

Get Our Newsletter